The landscape of women’s healthcare in the United States is currently facing a dual challenge: while medical technology has never been more advanced, public confusion regarding life-saving protocols has reached a critical peak. Statistics indicate that approximately one in eight women will develop invasive breast cancer during their lifetime. As one of the deadliest malignancies affecting women, the disease claims more than 42,000 lives annually in the U.S. alone. Despite the high stakes, recent surveys reveal a troubling disconnect, with 50% of women reporting significant confusion over current screening guidance. This uncertainty is not the result of a lack of interest, but rather the consequence of shifting and often conflicting recommendations from major medical organizations.
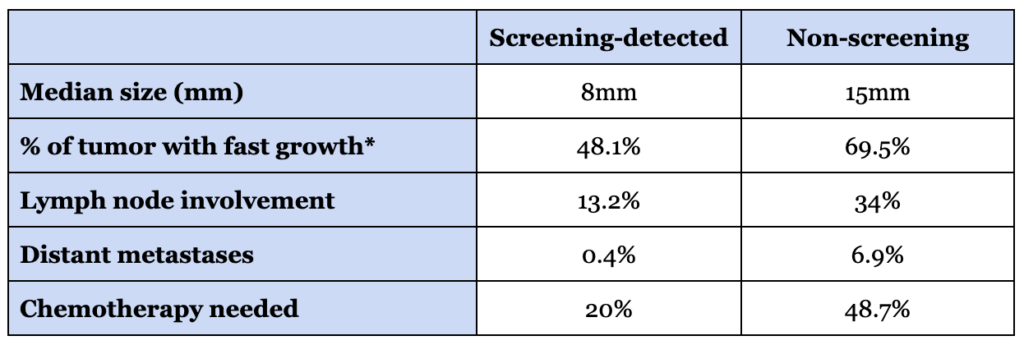
Medical experts emphasize that regular screening remains the most potent weapon against mortality. Women who adhere to consistent screening schedules are between 25% and 42% less likely to succumb to the disease than those who do not. Cancers identified through routine imaging are typically caught in early, localized stages—before they have metastasized—and are generally about half the size of cancers detected symptomatically. However, the persistence of high mortality rates suggests that the current implementation of these tools is failing to reach its full potential.
The Evolution of Screening: A Chronology of Guidance and Technology
The history of breast cancer screening has been marked by rapid technological advancement followed by lagging administrative consensus. In 2000, the Food and Drug Administration (FDA) approved the first full-field digital mammography (FFDM) system, moving the industry away from traditional film. A decade later, in 2011, the introduction of digital breast tomosynthesis (DBT), or 3D mammography, offered a more nuanced view of breast tissue, significantly reducing false positives and improving detection in dense tissue.
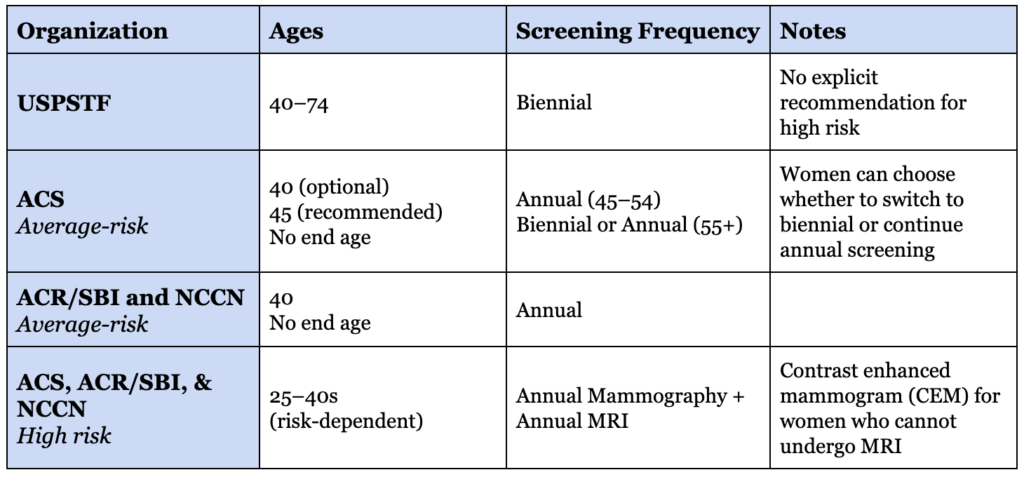
Parallel to these technological leaps, the guidelines governing their use have fluctuated. The U.S. Preventive Services Task Force (USPSTF), which often influences insurance coverage, has historically leaned toward more conservative "population-level" efficiency, recently recommending biennial (every other year) mammography for average-risk women aged 40 to 74. Conversely, groups such as the American College of Radiology (ACR), the Society of Breast Imaging (SBI), and the National Comprehensive Cancer Network (NCCN) advocate for annual screening starting at age 40.
This divergence has created a fragmented healthcare experience. While the USPSTF focuses on minimizing the "harms" of over-diagnosis and the cost-burden on the healthcare system, clinical organizations prioritize the "individual-level" benefit of maximizing survival odds. The result is an implementation gap where many women are either under-screened or screened with modalities that do not match their specific biological risk profile.
Identifying the Implementation Failure
The most glaring evidence of this implementation failure lies in the utilization of advanced imaging for high-risk populations. Clinical guidelines suggest that at least 9% of women meet the medical criteria for supplemental breast MRI (Magnetic Resonance Imaging) due to high lifetime risk or dense breast tissue. However, actual utilization rates hover at a staggering 0.4%. This means that fewer than 5% of women who should be receiving more intensive screening are actually doing so.
This discrepancy is rarely a failure of technology or a lack of diagnostic criteria. Instead, it is a failure of personalized medicine. Most women are placed into a default screening category without a formal assessment of their unique risk factors. Experts argue that moving away from a one-size-fits-all model toward a "risk-matched" protocol is the only way to significantly reduce the 42,000 annual deaths that currently occur despite the existence of effective screening tools.
The Framework for Personalized Risk Assessment
To close the gap between guidelines and clinical reality, medical professionals are increasingly advocating for a structured framework of personal risk assessment. This process begins with a formal evaluation, often utilizing the Tyrer-Cuzick model, which integrates family history, personal health factors, and breast density to calculate 10-year and lifetime risk estimates.
Genetic and Hereditary Factors
While only 5% to 10% of breast cancers are caused by known inherited mutations, their impact is profound. Pathogenic mutations in genes such as BRCA1, BRCA2, PALB2, ATM, and CHEK2 can increase lifetime risk to as high as 70%. Furthermore, these mutations often trigger more aggressive subtypes of cancer at much younger ages. While BRCA mutations occur in approximately 1 in 400 people in the general population, the frequency increases to 1 in 40 for those of Ashkenazi Jewish descent, highlighting the necessity of ancestry-informed screening.
The Challenge of Breast Density
One of the most significant yet overlooked risk factors is breast density. Approximately half of all women of screening age have dense breast tissue, which presents a dual problem: it independently increases the risk of developing cancer and makes mammograms significantly harder to read. On a standard X-ray, both dense tissue and tumors appear white, effectively allowing malignancies to "hide" in plain sight. Recent FDA mandates now require facilities to report breast density to patients, a critical step in informing women that they may require supplemental imaging beyond a standard mammogram.
Ancestry and Socioeconomic Variables
Data shows that non-Hispanic White women have the highest overall incidence of breast cancer, but Black women are more likely to be diagnosed at younger ages and with more aggressive, triple-negative subtypes. This disparity suggests that for certain populations, beginning screening at age 40 may already be too late to intercept the most lethal forms of the disease.
Comparative Performance of Imaging Modalities
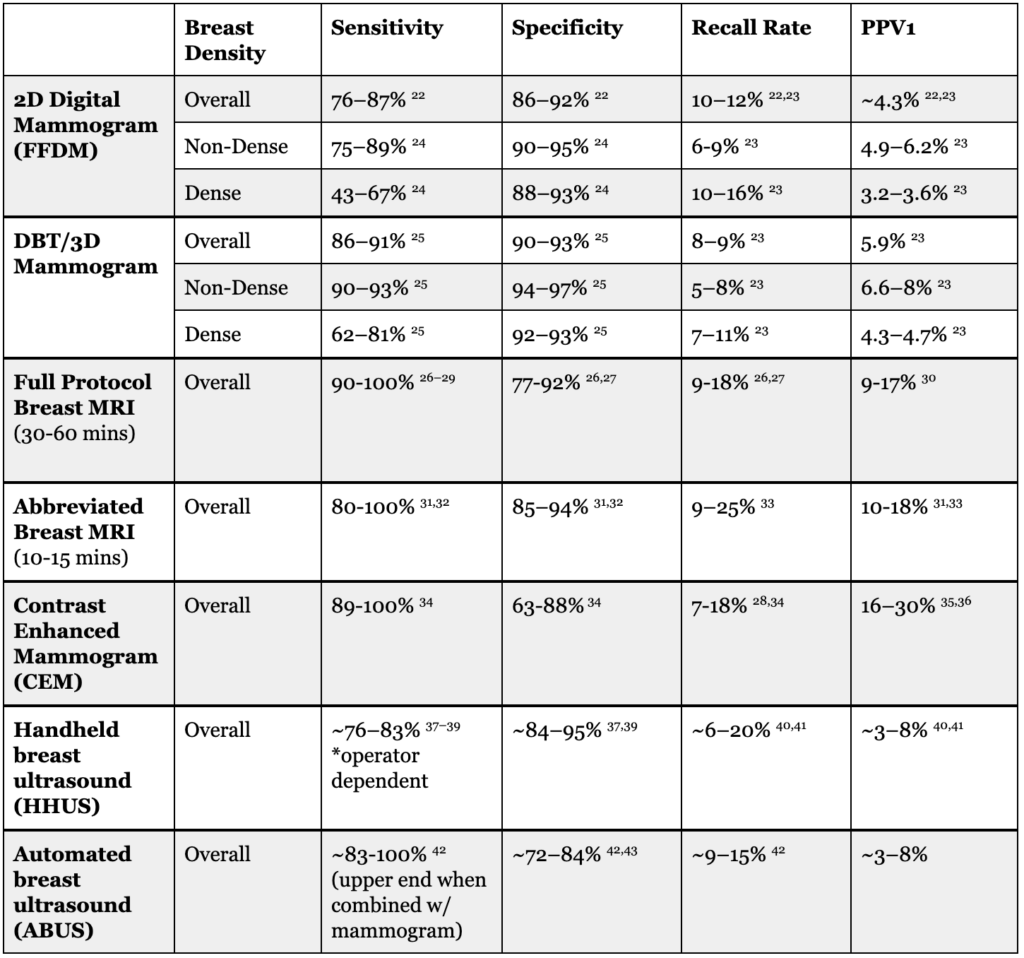
The choice of imaging tool is the most practical component of a risk-matched strategy. While mammography remains the bedrock of screening due to its ability to detect calcifications (often indicative of Stage 0 or DCIS), other modalities offer superior sensitivity for specific cases.
- 3D Mammography (DBT): This is now considered the superior standard over 2D digital mammography. By taking images from multiple angles, it allows radiologists to see through layers of tissue, increasing cancer detection rates and decreasing the number of "callbacks" for false positives.
- Breast MRI: As the most sensitive tool available, MRI is ideal for detecting small, invasive tumors. The development of "abbreviated MRI" protocols has reduced the time required for the scan from an hour to roughly 15 minutes, making it a more scalable option for women with high risk or extremely dense breasts.
- Contrast-Enhanced Mammography (CEM): This emerging technology combines traditional X-ray with an iodine-based contrast agent. It provides functional information similar to an MRI but at a lower cost and with greater accessibility, serving as a vital middle ground for women who cannot undergo MRI due to pacemakers or claustrophobia.
- Ultrasound: While highly operator-dependent, ultrasound remains a valuable supplemental tool, particularly in resource-limited settings or as a secondary check for suspicious findings on a mammogram.
The Burden of False Positives
A major point of contention in public health circles is the "false positive" rate. In the United States, roughly 10% of screening mammograms result in a "callback" for additional testing. Of those, only about 5% lead to a cancer diagnosis. Over a decade of annual screening, more than half of all women will experience at least one false positive.
The psychological and logistical toll of these callbacks—ranging from anxiety to time lost from work—is often cited by the USPSTF as a reason to screen less frequently. However, from a journalistic and clinical perspective, the weight of this "harm" is relative. For a woman at high risk, the "burden" of a follow-up biopsy is often viewed as an acceptable trade-off for the early detection of a life-threatening tumor. For an average-risk woman, the calculation may differ. This highlights why "risk-matched" screening is not just about finding more cancer, but about ensuring the intensity of the screening matches the probability of the disease.
Implications for Future Public Health Policy
The current state of breast cancer screening in the U.S. suggests a need for a paradigm shift. Rather than debating whether women should start at 40 or 50, or screen every one or two years, the focus is moving toward identifying risk early. Experts now suggest that every woman should undergo a formal risk assessment by age 25. This allows for the identification of the "high-risk" minority who may need to begin MRI screening in their 20s or 30s, while allowing average-risk women to follow standard protocols with confidence.
Furthermore, the data regarding women under 40 reveals that risk factors are often more predictive than age. Women aged 35–39 with a single risk factor (such as dense breasts or family history) have a cancer detection rate three times higher than average-risk women in their early 40s. This evidence supports the argument that screening should be dictated by biology rather than the calendar.
Ultimately, the goal of modern breast cancer screening is to transition from a passive, age-based system to a deliberate, risk-based strategy. By aligning the right imaging tools with the right woman at the right intervals, the medical community can move closer to eliminating preventable deaths from a disease that remains one of the most significant threats to women’s health worldwide. Consistent adherence to a personalized plan, informed by genetic, architectural, and lifestyle factors, represents the most effective path forward in the ongoing effort to improve survival outcomes.