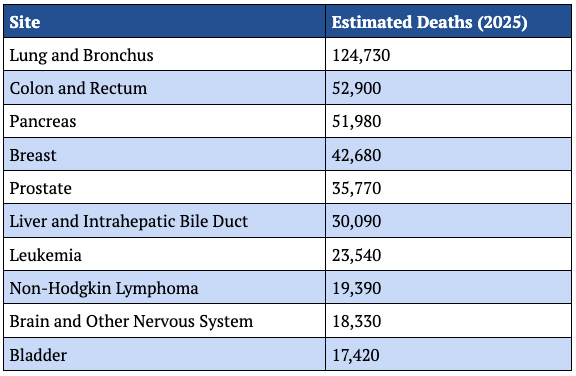
The landscape of oncological preventative care is currently facing a profound paradox: despite the existence of highly sophisticated imaging technologies and a deeper understanding of tumor biology, breast cancer remains the leading cause of cancer-related death for women globally. Recent projections from the Surveillance, Epidemiology, and End Results (SEER) program indicate that breast cancer will continue to be a primary driver of mortality through 2026, claiming tens of thousands of lives annually. This persistent mortality rate has prompted medical experts, most notably Dr. Peter Attia and various radiological societies, to call for a fundamental shift from standardized, population-based screening guidelines to a more rigorous, personalized framework. The objective of this new strategic approach is to bridge the gap between theoretical screening efficacy and actual clinical outcomes by emphasizing individual risk profiles over broad age-based mandates.
The Current Crisis of Under-Screening and Mortality
The fundamental question facing the medical community is why mortality remains high when early-stage detection carries a nearly 100% five-year survival rate. Data suggests that the issue is twofold: a failure in the consistency of screening and a failure in the intensity of screening for high-risk individuals. While population-level guidelines are designed to balance the benefits of cancer detection against the harms of over-diagnosis and "false positives," these broad strokes often leave the most vulnerable women under-protected.
A critical metric highlighting this systemic gap is the utilization of Magnetic Resonance Imaging (MRI). Clinical criteria suggest that approximately 9% of the female population meets the high-risk threshold for supplemental MRI screening. However, actual utilization rates remain stagnant at a mere 0.4%. This staggering discrepancy indicates that the majority of women who would benefit most from high-sensitivity imaging are only receiving standard mammography, which may be insufficient for their specific biological profiles. Furthermore, inconsistent screening—skipping years or starting late—significantly erodes the cumulative benefit of early detection. Studies have shown that women who undergo regular, consistent screening are up to 40% less likely to die from the disease compared to those who do not.
A Chronology of Evolving Guidelines
The history of breast cancer screening recommendations is marked by frequent shifts and often contradictory advice from major medical organizations. For decades, the baseline for screening was set at age 50. However, as data emerged regarding the rising incidence of cancer in younger cohorts, organizations began to diverge.
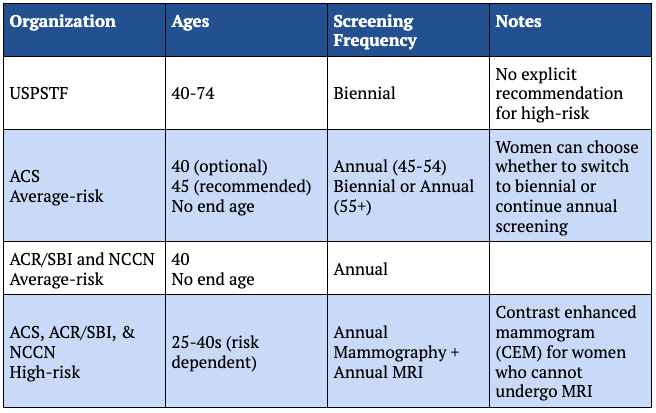
In the early 2000s, the U.S. Preventive Services Task Force (USPSTF) stirred controversy by suggesting that women aged 40 to 49 should make individual decisions rather than follow a blanket recommendation for annual mammography. By contrast, the American College of Radiology (ACR) and the Society of Breast Imaging (SBI) have long maintained that annual screening should begin at age 40 for all women of average risk. In 2024, the USPSTF updated its guidance to recommend biennial (every two years) screening starting at age 40, a move that many experts argue still falls short of the optimal annual cadence required to catch aggressive, fast-growing tumors.
This evolution reflects a tension between public health economics—where the goal is to minimize the cost and anxiety of false positives across millions of people—and individual clinical excellence, where the goal is to ensure no cancer goes undetected. The emerging consensus among specialists is that the "middle ground" offered by population guidelines is often an inadequate fit for the individual.
The Biological and Genetic Drivers of Risk
To move toward a personalized model, patients and providers must first quantify baseline risk using a variety of vectors. Genetics remains the most potent factor; mutations in the BRCA1 and BRCA2 genes significantly increase the lifetime risk of breast cancer, often shifting the window of onset into a woman’s 20s or 30s. However, family history serves as a critical proxy even in the absence of known mutations, reflecting shared environmental factors and polygenic risk scores that current single-gene tests may miss.
Beyond genetics, breast density has emerged as a primary concern for both risk and detection. Approximately 50% of women of screening age have "dense" breast tissue, which is composed of more glandular and fibrous tissue than fatty tissue. This density is a double-edged sword: it is an independent risk factor for developing cancer and it creates a "masking effect" on traditional 2D mammograms. On an X-ray, both dense tissue and tumors appear white, making the detection of small masses akin to finding a "snowball in a blizzard." The FDA’s recent mandate requiring imaging centers to notify women of their breast density is a significant step toward informed, personalized decision-making.
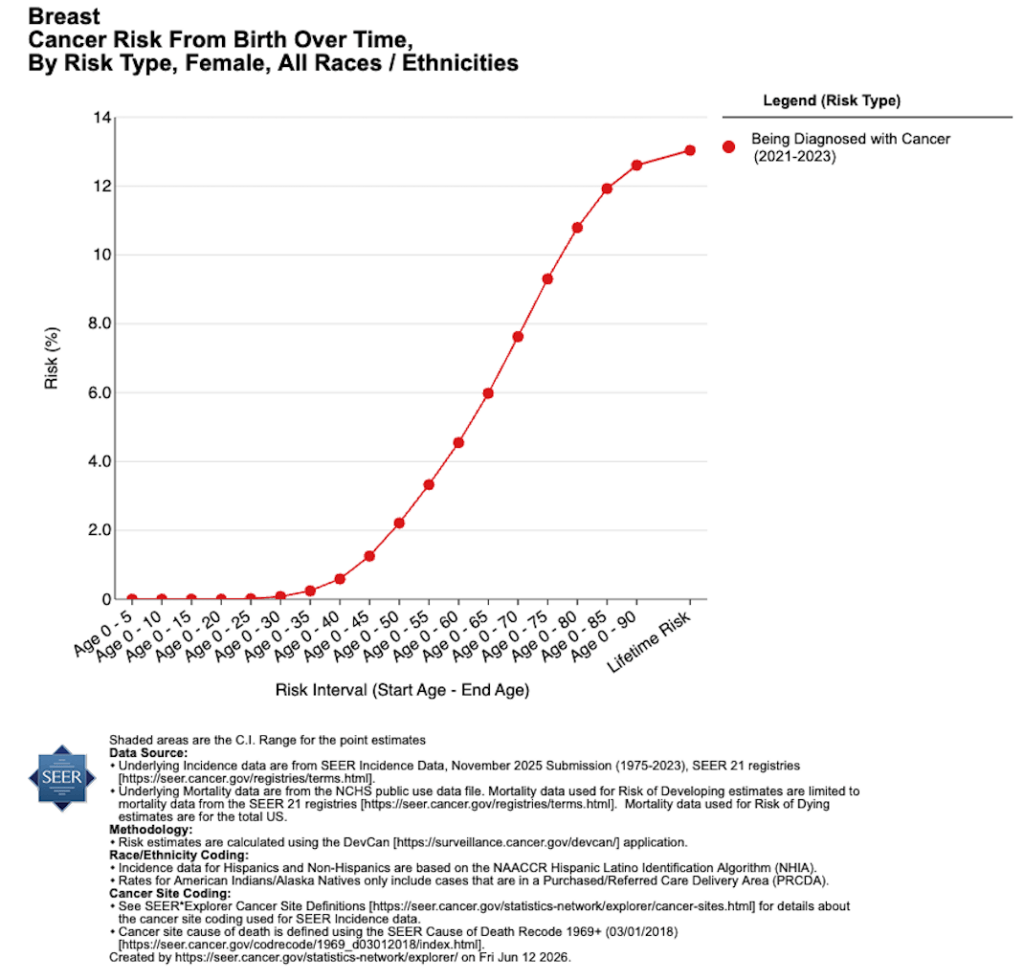
Other factors, including reproductive history (age of first pregnancy, breastfeeding duration), lifestyle choices (alcohol consumption, metabolic health), and prior chest radiation for unrelated conditions (such as Hodgkin’s lymphoma), must be integrated into risk calculators like the Tyrer-Cuzick or Gail models. When a woman’s lifetime risk exceeds 20%, she is generally classified as "high risk," necessitating a screening protocol that goes beyond the standard annual mammogram.
Technological Modalities: Expanding the Toolkit
Modern breast imaging is no longer a monolithic field. It is a hierarchy of tools, each with specific strengths and limitations:
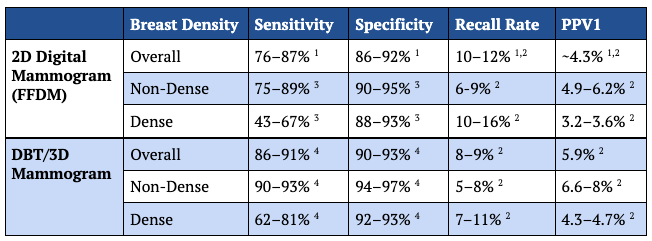
- Digital Breast Tomosynthesis (3D Mammography): Now considered the baseline for modern care, 3D mammography takes multiple images from various angles to reconstruct a three-dimensional view of the breast. This significantly reduces the recall rate and increases the detection of invasive cancers, particularly in women with moderately dense breasts.
- Magnetic Resonance Imaging (MRI): MRI is the most sensitive tool available, capable of detecting cancers that are invisible on mammography. While it has a higher rate of false positives, its ability to find aggressive tumors at their earliest stages makes it indispensable for high-risk patients.
- Contrast-Enhanced Mammography (CEM): An emerging alternative to MRI, CEM involves the injection of an iodine-based contrast agent to highlight areas of increased blood flow associated with tumor growth. It offers functional information similar to an MRI but at a lower cost and with greater accessibility.
- Ultrasound: Often used as a supplemental tool for women with dense breasts, ultrasound is highly dependent on the skill of the technician. While useful, it is generally viewed as secondary to MRI or CEM in terms of sensitivity.
The Debate Over Frequency: Annual vs. Biennial
One of the most contentious points in breast cancer screening is the interval between tests. The Cancer Intervention and Surveillance Modeling Network (CISNET) has provided extensive data comparing annual and biennial (every two years) schedules. The findings are clear: if the primary goal is the reduction of mortality, annual screening is superior.
Modeling data shows that annual screening for women aged 40 to 79 results in a 42% reduction in mortality, whereas biennial screening results in only a 30% reduction. The argument for biennial screening is almost entirely centered on reducing the "harm" of false positives—instances where a woman is called back for additional imaging or a biopsy for a finding that turns out to be benign. However, clinical analysis suggests that for many women, the trade-off of a 12% difference in mortality is a price too high to pay for the avoidance of a temporary period of anxiety following a callback.
Screening in Younger Populations
While breast cancer is less common in women under 40, the tumors that do appear in this age group are disproportionately aggressive. Approximately 20% of cancers in women under 40 are "triple-negative," a subtype that grows rapidly and lacks the receptors targeted by many common therapies.
For women with high-risk genetic profiles, screening must often begin as early as age 25, typically with annual MRI. For women of average risk, there is a growing argument for a "baseline" mammogram in the mid-30s. The purpose of this baseline is not necessarily to find cancer, but to establish the patient’s breast density. Knowing one’s density early allows for the design of a screening strategy that might include supplemental ultrasound or MRI once formal annual screening begins at age 40.
The Limitations of Screening: Symptomatic Disease
A critical distinction in oncology is the difference between screening (for asymptomatic people) and diagnostic evaluation (for those with symptoms). A common and dangerous misconception is that a recent "clear" mammogram rules out the possibility of new symptoms being cancerous.
Inflammatory Breast Cancer (IBC), for example, is a rare but highly aggressive form of the disease that often does not present as a lump and may not be visible on a standard screening mammogram. It typically presents as skin redness, swelling, or a "pitted" texture similar to an orange peel. Because IBC spreads through the lymphatic vessels in the skin, it requires immediate diagnostic intervention, regardless of when the patient’s last screening occurred. This highlights a vital rule of breast health: any new symptom—a lump, discharge, or skin change—must be evaluated promptly, even in men, who account for approximately 1% of all breast cancer cases.
Conclusion: Toward a Personalized Future
The transition from a passive, guideline-reliant approach to an intentional, risk-based strategy is the most promising path toward reducing breast cancer mortality. The "one size fits all" model of public health is increasingly at odds with the capabilities of modern medicine.
To optimize outcomes, the medical community and patients must prioritize three actions: early and accurate risk assessment, the selection of imaging modalities based on breast density and genetic profile, and a commitment to annual consistency. While systemic barriers such as insurance coverage and access to specialized imaging centers remain, the individual’s power lies in the transition from being a subject of population-level statistics to an informed manager of their own biological risk. The tools to prevent breast cancer death exist; the challenge remains in their precise and personalized application.